
Request an Appointment

BY PHONE
by Rosalina Mahendran MScPT
Registered Physiotherapist
updated Mar 11, 2026
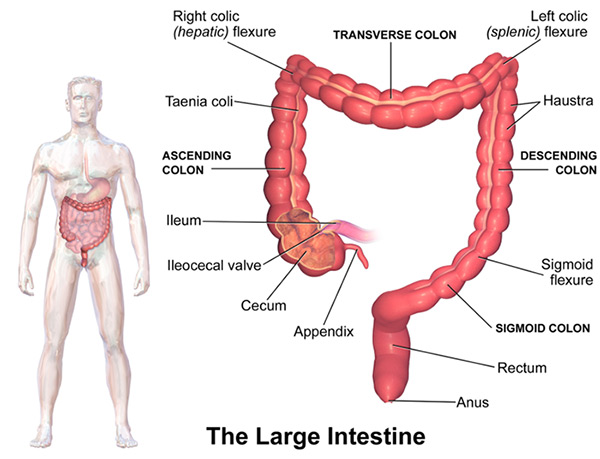
Colorectal cancer is a malignant tumour that most often starts in the cells of the colon or rectum, which are parts of the large intestine and digestive system. These structures play an essential role in processing and eliminating waste from the body.
Colorectal cancer is one of the most common cancers in Canada. Approximately 6% of Canadians will develop colon cancer during their lifetime, making it the fourth most common cancer and the second leading cause of cancer-related death in the country (likely due to a higher rate of younger individuals developing this type of cancer).
The encouraging news is that colorectal cancer is highly treatable when detected early, which makes awareness and screening extremely important. Physiotherapy, particularly pelvic floor physiotherapy, can also play an important role in supporting recovery before and after colorectal cancer treatment.
Signs and Symptoms of Colorectal Cancer
Some common signs and symptoms include:
- Changes in bowel habits (constipation, diarrhea, or changes in stool consistency)
- Rectal bleeding
- Blood in the stool
- Abdominal discomfort such as cramps, gas, or pain
- A persistent feeling that the bowel does not fully empty
- Weakness or fatigue
If you experience any of these symptoms, it is important to speak with a healthcare provider.
Rectal Cancer and Surgical Treatment
Treatment for colorectal cancer depends largely on where the tumour is located.
If the cancer is located in the upper portion of the rectum, surgeons may remove the affected section and reconnect the colon to the remaining rectum. In many cases, bowel function can return relatively close to normal after recovery.
For cancers located lower in the rectum, surgery may require removal of both the rectum and the anus. In these cases, a permanent colostomy may be required to allow waste to exit the body.
Some patients may also receive a temporary stoma during treatment. A stoma is an artificial opening created in the abdomen that allows stool to pass into an external pouch while the bowel heals after surgery.
Types of stomas include:
- Colostomy – created from the colon
- Ileostomy – created from the small intestine
Temporary stomas may be used to help prevent complications such as anastomotic leaks (when the bowel/intestine fails to connect properly) or bowel obstruction during the healing process.
Types of Colorectal Surgery
Surgery is the primary treatment for colorectal cancer and typically involves removing the diseased section of the intestine.
Local Excision or Local Resection
This procedure removes small early-stage tumours or polyps located on the lining of the colon or rectum. It may also be used to remove a local recurrence of a tumour and relieve symptoms such as pain.
Bowel Resection (Most Common Procedure)
This surgery removes a section of the bowel along with nearby lymph nodes.
Types of bowel resections include:
- Right hemicolectomy – removal of the right side of the colon
- Transverse colectomy – removal of the middle portion of the colon
- Left hemicolectomy – removal of the left side of the colon
- Sigmoid colectomy – removal of the final section of the colon
- Lower anterior resection – removal of the lower colon and part of the rectum
- Proctocolectomy – removal of the rectum and part of the sigmoid colon
- Abdominoperineal resection – removal of the rectum, anal canal, and surrounding muscles
- Subtotal colectomy – removal of most of the colon
- Total colectomy – removal of the entire colon
In some cases, surgeons may also perform an omentectomy, which removes the omentum, a fatty fold of tissue in the abdomen that helps protect the organs.
Low Anterior Resection Syndrome (LARS)
Many individuals who undergo surgery for rectal cancer, particularly a lower anterior resection may develop a group of bowel symptoms known as Low Anterior Resection Syndrome (LARS).
The rectum normally holds stool, helping regulate bowel movements. When part of the rectum is removed, this storage capacity is reduced, which can lead to changes in bowel function.
Common symptoms of LARS include:
- Incontinence
- Frequent bowel movements
- Fecal Urgency (a sudden need to use the bathroom)
- Problems with gas/stool differentiation
- Multiple bowel movements within a short period
- A feeling of incomplete bowel emptying
Management strategies may include dietary modifications, bowel retraining strategies, medications, and pelvic floor physiotherapy.
Risk Factors for Colorectal Cancer
Most colorectal cancers are not hereditary, but several factors can increase risk.
Genetics and Family History
If a parent or sibling has had colon cancer, the lifetime risk increases to approximately 10–12%.
Certain inherited conditions account for about 5% of colorectal cancer cases, including:
- Familial adenomatous polyposis (FAP)
- Lynch syndrome
- Gardner’s syndrome
Medical Conditions
Long-standing inflammatory bowel conditions can also increase risk, including:
- Ulcerative colitis
- Crohn’s disease
- Inflammatory bowel disease
Lifestyle Factors
Additional risk factors include:
- Obesity
- Colon polyps
- Smoking and alcohol use
- Diets high in red or processed meats
- Low fibre intake
- Cooking meats at very high temperatures
Colorectal Cancer Screening
Colorectal cancer is most treatable when detected early, making regular screening extremely important.
In Canada, routine screening is recommended for individuals between ages 50 and 74 who do not have additional risk factors. However, healthcare providers are increasingly seeing younger individuals developing colorectal cancer, making awareness even more important.
Common Screening Tests
Fecal Occult Blood Test (FOBT or FIT)
An at-home stool test that checks for hidden blood in the stool. It is typically performed every two years.
If this test is abnormal, a colonoscopy is usually recommended to investigate further.
Other screening options may include:
- Flexible sigmoidoscopy
- Colonoscopy
- Endoscopy
The Role of Physiotherapy in Colorectal Cancer Care
Physiotherapy can play an important role both before and after colorectal cancer treatment.
Prehabilitation (Before Surgery)
Research shows that entering surgery in better physical condition can significantly improve recovery outcomes.
Prehabilitation programs may include:
- Pelvic floor muscle training
- Cardiovascular conditioning
- Strength training
- Education about bowel health and recovery
Research suggests that patients who perform supervised pelvic floor exercises before rectal surgery may experience lower rates of fecal incontinence after surgery (Lin et.al , 2015). Poor preoperative anal sphincter function has also been identified as a predictor of Low Anterior Resection Syndrome (LARS) (Christnessan et al, 2020)
Common Cancer Side-Effects Physiotherapy Can Help Treat
Cancer-Related Fatigue
Fatigue is one of the most common side effects during and after cancer treatment. Structured cardiovascular and exercise programs can help improve energy levels and physical function.
Chemotherapy-Induced Peripheral Neuropathy
For a detailed look at CIPN click here.
Muscle Weakness and Postural Changes
After surgery or treatment it is common for individuals to develop a forward or hunched posture, which can contribute to:
- Difficulty breathing
- Slower digestion
- Increased joint pain
- Balance challenges
Physiotherapy treatment may include:
- Postural strengthening exercises
- Breathing exercises
- Manual therapy for thoracic spine mobility
- Progressive strength & functional training programs
Survivorship
A recent research study conducted by the Canadian Cancer Trials Group (CCTG) known commonly as the CHALLENGE trail found that a structured exercise program initiated soon after chemotherapy for colon cancer resulted in significantly longer disease-free survival and overall survival. (Courneya et al, 2025).
Scar Tissue and Soft Tissue Restrictions
- Abdominal scar tissue mobilization
- Soft tissue techniques
- Targeted mobility exercises
Bowel, Bladder, and Sexual Health Dysfunction
Pelvic floor physiotherapy can help address:
- Fecal urgency/frequency or incontinence
- Difficulty emptying the bowel
- Bladder dysfunction
- Pelvic pain/Sexual dysfunction
Treatment strategies may include:
- Pelvic floor muscle training
- Biofeedback therapy using Balloon Catheter Training
- Toileting mechanics education
- Fibre and bowel diaries
- Dilator therapy
- Internal and external soft tissue treatment
- Strength Training (general and abdominal)
- Tibial nerve stimulation

Lymphedema
The pelvis contains many lymph nodes, and colorectal cancer treatment can sometimes lead to lymphedema, which is swelling caused by a buildup of lymph fluid.
Click here for a detailed look at Preventing Lymphedema After Breast Reconstruction: Why Early Physiotherapy Matters
When Should Someone See a Physiotherapist After Colorectal Surgery?
Many people assume physiotherapy is only needed if they develop symptoms, but early rehabilitation can significantly improve recovery.
You may benefit from seeing a physiotherapist if you experience:
- Bowel urgency/frequency or difficulty controlling bowel movements
- Constipation or difficulty emptying the bowel
- Symptoms of Low Anterior Resection Syndrome (LARS)
- Pelvic pain or discomfort after surgery
- Abdominal tightness or scar tissue restrictions
- Weakness, fatigue, or reduced physical activity
A physiotherapist trained in both oncological and pelvic health rehab can help guide recovery, improve bowel function, and support a return to normal daily activities.
How our Registered Dieticians can help
Colorectal cancer treatments often cause changes not only in digestion but also food tolerance/sensitivities. Our Registered Dieticians are a key resource for survivors of colorectal cancer. They can help you to navigate these new changes/norms to understand and control them better so they are less disruptive to your life. Learn more how they can help here
Supporting Recovery and Quality of Life
Recovering from colorectal cancer treatment often involves more than just healing from surgery. Many individuals experience changes in bowel function, strength, mobility, and energy levels.
If you are experiencing bowel changes, pelvic discomfort, or weakness after colorectal surgery, working with a pelvic health physiotherapist may be an important step in your recovery journey.


Questions? We're happy to help!
Choosing the right service provider can be a big decision. We’re dedicated to answering any questions you have to help you make the best choice. Contact us today and ask us anything!
Call us at (416) 238-6749