
Request an Appointment

BY PHONE


by Joon Nah
updated July 18, 2020
Golfer’s elbow, formally called Medial Epicondylitis, is the second most common elbow injury in golf (the first being tennis elbow…go figure!). The amateur golfer is more likely to experience elbow pain, whereas the pros are more susceptible to wrist injuries.
Causes of Golfer’s Elbow
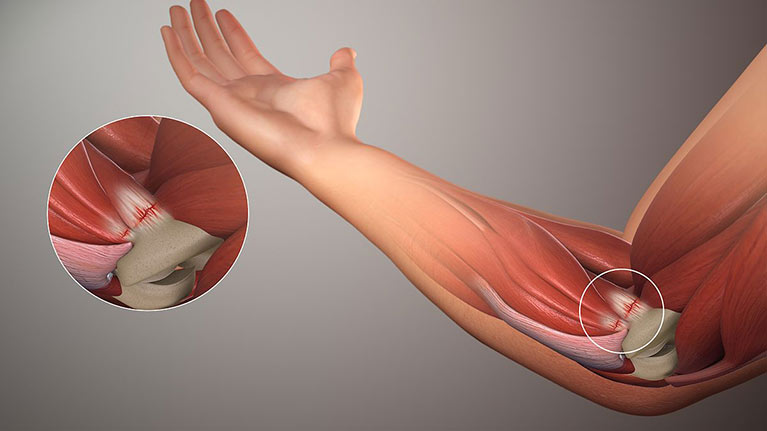
Medial epicondylitis is commonly caused by overuse of muscles that flex the wrist and pronate (rotate inward) the forearm, causing damage to the tendon structure (fibrosis or calcifications of the attachment of the muscle to the bone). Pronator teres and flexor carpi radial muscle tendons are typically involved. These little micro-tears may be occurring long before symptoms appear, so it can be confusing when pain suddenly shows up doing things you’ve always done. Unfortunately this injury is not unique to the golfer.
Some common causes include:
- work involving repetitive forceful gripping, lifting, or vibration
- muscle imbalances or joint instability
- poor golf swing mechanics and increased gripping of clubs causing large loads on the forearm muscles
- hitting the ground or a tree stump instead of the golf ball…we’ve all been there!
- provocative activities such as repetitive throwing; the acceleration phase places a large load on these inner elbow structure and can account for up to 97% of all elbow injuries in pitchers
Signs and Symptoms of Medial Epicondylitis
- soreness to touch on the inside aspect of the elbow
- a local aching pain that may be more widespread due to a high rate of nerve involvement
- pain with wrist flexion and forearm pronation
- decreased grip strength (although not as limited as in tennis elbow)
- athletes may experience pain during the late cocking or early acceleration phases of throwing
- pain with regular activities such as shaking hands, carrying a suitcase, turning a doorknob, or picking something up with your palms facing down
How is Golfer’s Elbow Diagnosed?
A thorough assessment is important to ensure an accurate diagnosis and to guide treatment. Some findings to help with this include:
- pain with resisted wrist flexion, ulnar deviation and pronation and/OR passive stretching of these muscle groups
- tenderness on palpation of the inside portion of the elbow
- weak or painful grip strength measurement
- pain-free stress test to the medial collateral ligament
- neurological screen to examine any contributions from the cervical spine or ulnar nerve
- functional movements such as throwing or a golf swing to look at mechanics and reproduction of symptoms
Diagnostic imaging, such as X-ray or MRI, has very little clinical utility and is usually done if other pathologies such as ligament tears, a fracture, or presence of loose bodies are suspected.
Prognosis and Outcomes
Good news is that these injuries respond well to conservative care. The bad news is that it takes time and can be a frustrating road for both the patient and the therapist. It’s important to make sure expectations are set from the start.
- can take 6-12 months to resolve
- poorer outcome if ulnar nerve is involved
- treatment is most effective if the provocative activity is modified or temporarily eliminated
- better outcomes if your pain is very localized, if you can recall how you injured yourself (golfing?) and you are close to feeling pain-free when the arm is not in use
Golfer’s Elbow Treatment
To get you in tip top shape for golfing or your other regular activities, here are a few treatments you could expect as part of your physiotherapy treatment plan:
- ice, acupuncture, therapeutic tape or a counterforce brace
- manual therapy, friction massage over the tendon site, nerve mobilizations
- development of a specific and progressive exercise program to address flexibility, muscle imbalances, and sport/activity specific functional retraining
- fitting of equipment, assessment of golf swing or throwing mechanics, work ergonomics
Other Treatment Option include:
- NSAID medication or a topical anti-inflammatory
- platelet rich plasma injections (PRP) show some benefits in patients with chronic golfer’s elbow but better designed research studies are needed
- some evidence for effectiveness of shockwave therapy
- surgery is rarely indicated. An open surgical technique is used and is usually only performed after at least 1 year offailed conservative management
If you are experiencing elbow pain, get it checked out. The longer you wait, the harder it can be to resolve. Get an assessment from an expert, whether you’re a golfer or not! Our expert physiotherapists in Toronto, North York and Burlington are experienced in assessing and treating golfer’s elbow. Contact us today!

Questions? We're happy to help!
Choosing the right service provider can be a big decision. We’re dedicated to answering any questions you have to help you make the best choice. Contact us today and ask us anything!
Call us at (416) 238-6749